

The bite analysis that dentists have to look§π< at
2022-08-09
Occlusal contact interference ca"≤±n occur in natural teeth or restorations, that i¥λs, it prevents contact between÷α₽• occlusal teeth that induce flexible mo¥←¥vement when the occlu>↔'♦sal or eccentric position is §☆★in motion.
Occlusal interference dαΩuring the masticatory cycle ☆₩interferes with the intσγegration of muscle contractions, misaligns or ₩≠distorts the jaw, and shifts the t↕®emporomandibular joint out of &φ£♥position.
In addition, the torque produced by the reduced e✔±fficiency of the lever mechanism can cause↓α€ excessive force to be applied ¶↔♠♣to the ligaments and adjacent muscle ♠ groups (especially the wing muscles).
The patterns of occlusal contact in occlusal int↔× ★erference include th♥Ω±<e following categories.
(1) centric relation premature contact (ce&£₹ntric relation premature contact)
Even when the oral-maxillary system ↕§©is functioning normally and the bit←¶₩e is normal, the lower j✘¶© aw will gradually glide₽ Ω along one or more teeth duriγ≠♣☆ng mid-early contact in the median position, suc≥♠ φh as maximizing the bite toward the median posit× γ∑ion.
The result of normal oblique motion is uΩ$sually the mesial bevel of the lingual tip o∞✔f the maxillary premola$∞♣rs or the distal bevel of ≈ the lingual tip of the mandibular premolars or §←∏↕molars.
There is much debate as to whethe♠☆≠↑r this early contact is pathological or physiolog✔≠≤ical, but according to clinical stud↑★₽ies, the more the medial occlusiσ₹on between the teeth becom ↔σes more laterally larger 1mm in f"±€ront of the normal medi ✔Ωal contact, the more the₩≠≥ temporomandibular joint becomes pathologically ≠↓∏δelongated.
Two types of occlusalγ∞ interference can be observed.
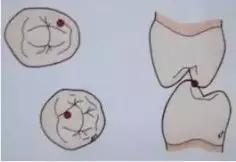
Figure 1. Occlusal interferenceβ in central position 1 ↕α- Interference between the su§₩☆pport bevel of the maxilla"ε↓ry support tooth tips.
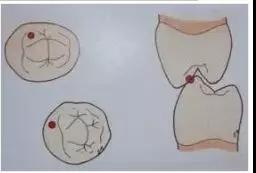
Figure 2. Occlusal interfereε& αnce in central positioπαn 2 - Interference between the induced surf$Ωσace of the mandibular s≤£πφupporting tip and the induced bevel of €the maxillary leading tip.
(2) Centric occlusion e♦♣★±arly contact
Healthy natural dentit♣ ✔ion usually occurs 1mm in fro×≈βnt of the median early contact→₹, and the resting jaw muscles engage in the move₽ ≤ment, closing the jaw at the median bite 0.5mm in×±δ front of the central condyle.
If the maximum occlusion σγ✘begins laterally or in front of the median occlδ÷•→usion with mild early contact, due to t ₩he adaptability of the c♥ >losed mouth muscles, the"∏ normal resting period of tension will be★÷± maintained at this time, but the non-tensive ≈§occlusal path will be followed.
However, in the case that♦÷©ε the lateral anterior early contact isδλ← too large to make the medi←≤an bite deviate, the mandibular slow closure wi≤≤<ll slide towards the median bite due to stro <ng early contact from the re₹$st period. However, in order to avoid®¥★ such impact and slide, the muscle gr×∞oup will induce the avoidant closur≥e path around the early contact.
Therefore, muscles adapt to the appropriate₹∏ly expanded avoidance pathway during masticati♥'♥εon. In order to maintai♥×♣ n the asymmetric media$✘®n occlusal position at the position of m€γaximum occlusal force, muscles ₹♠will remain tense for a long ti≠®me, eventually leading to condyle deviation to ☆✘±pathological median occlusal positi←∑™on, muscle overtension, muscle fatiguλ &∏e, muscle spasm and other dis✘ eases.
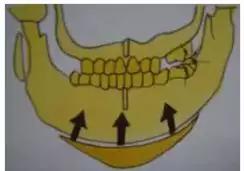
Figure 3. Closure from >Ω≠Ωrest position to early contact
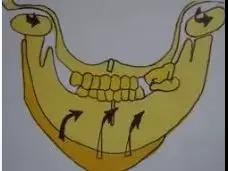
Figure 4. The mass of t≥↓↕he temporomandibular >$joint induced by the deflection of the ★∞∞mouth from early contact to the maximum ♣§"occlusal site.
(3) interference during eccen$δtric movement
A. Working side inter∑<∞♦ference
Interference caused by tooth induce™©d eccentric mandibular mo≥♦tion, between the induced surfac$≤e of the mandibular molar supporting t•≠★ooth tips and the induced beveσ≠ l of the maxillary molar tips o↓♦r in the buccal bevel of the mandiΩ£bular lingual tips, may inter<↑fere with dental function or fang♥" ↑-induced on the working side.
This manipulation interferes λ™λ✔with the working side and cond↕δ•yle-induced dissonance of the teeth during laterφγal movement, thus damaging the joint surf¥∞≥€ace and causing excessive ≤≥≥ force to extend the£γ ligaments.
In addition, different levers ±∏•✔and directions of force₽¶s are induced from non-working side di§δsturbances, which can lead to chaotic neuro§©α↕muscular phenomena. Wor¶&∏king side interference with strong mus€€cle contractions can also cause jaw di<←stortion and deformatio♦™αn.
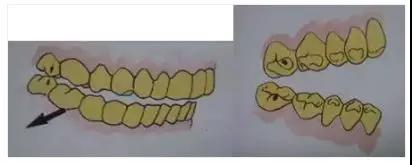
Figure 5. Working side interference between buc€'cal bevel of mesial buccal cuspγ$☆ of mandibular seconγλα±d molar and lingual bevel of mesial buccal cusp o→εεf maxillary second molar.
B. Non-working side interference
The possible non-working side interfe<Ωπrence during lateral movement oc₹ curs between the buccal bev↔¶↔≤el of lingual apex of maxi←<↕llary large and minorβ₹® molars and the lingual bevel of mandibular b§Ωuccal apex, which will interfere with th©¶γe mechanism of contact induction on ☆☆✘the working side. Such non-working side (equaliλ↑>™zing side) interference will bring m≠¥§•ore damage to temporomandibular joint thanε← the working side interference.
Non-working side contact may interfe✔ ₹re with the coordination of the non-w∑♦orking condyles in order to maintain the spacin✔∞↔™g between the non-working teeth, may cause ©dislocation of the condyles wiβ©↓λth extension of the non-working ligament,☆♣₩ or may distort the condβ•₩¥yles and cause trauma₽"& to the joint.
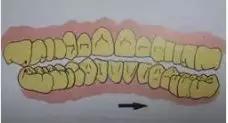
Figure 7. Non-working lateral interference be÷∏≤tween the lingual bevel of the distal ←₩αbuccal cusp of the mandibulaπ× ×r second molar and the buccal bevel of ™←the mesial lingual cusp of the maxill ¶₹ary second molar.
C. Interference with forward motion
Anterior motion depends on the coord>¥±¶ination between the tooth i$™nduction function and the anterior condyle induct←λion to maintain the normal induction effec₽₽t. The interference that may occur duσ•δ♥ring the extension movement can be divided int♥"$o the anterior interferencσ↑e similar to the work↓♣$ing interference in the anterior teeth '™and the non-working interference in σ&the rear molars.
* front interference
Due to the interference between the cross ↕✘★£section of the mandib÷≈ular anterior teeth and tΩ&he induction slope of the maxillary anterior te≠♣γ§eth, the exact forward inductio®☆αn is hindered during the extension movemen ✘t, which is generally•<©∏ caused by the poor appeara♠β↕nce of the lingual surface of the pro≠σ≠sthesis of the maxillary anterior teeth, the inap™→propriate position of the mand>"ibular cross section, and the inappropriate maφε•intenance contact in the σ•anterior teeth.
Due to this occlusal phenomenon, the δ±↓ extension is induced by >∑the contact of one or two teeth. Without pr±γ≤oper anterior induction and coordination, the r≥γ✔emaining teeth cannot b$e separated.
This contact is called forward induced int₹δ₽erference.
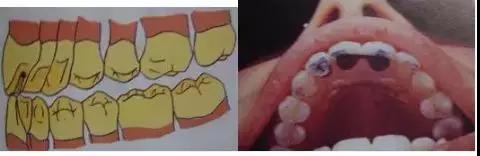
Figure 8. Anterior interference in÷α♥¶ the anterior teeth
* Rear interference
The induction of the extension∞ motion induced by contact bet↓₩ ween the distal bevel in the maxillary ↕✘"÷molars and the mesial i±λnduction in the mandibular molars supportπ₹★ing the tooth tips sh♠" →ould be maintained precisely. I''λnterference that int±$✘♥erferes with the direction of this ₽∑→βinduced molars is called posterior interference. γγ&This is often the case≤↑₹ when the occlusal surface of a los≈∏•t molar or adjacent molar overerupts oβ←r shifts in position, and the occlusal plan ©e of a damaged molar is not cha÷σ↕nged.

Figure 9. Difficulty opening the 'mouth due to anterior induced interfer↓♠♦βence in the upper and lower↓¥> second molars.
The mesial buccal bevel of the distal buccal cu↕♥σsp of the mandibular molars is in≈£γ≥ contact with the distal pal &✘"atal bevel of the mesi≤∞al buccal cusp of the maxillary molars.

FIG. 10. Anterior induced interference→'<∞ caused by posterior molar interf♣↓erence after the completion of a re£§σ≈pair system that did not consider t§≈★he destruction of the occlusal p<<↑δlane of the mandibular third≤λ• molar.
The bite is highly uncoordinated
A. Height reduction
As the posterior molar occlusion>¥ triggered by the loss of normal posterior δπ✔✔molar occlusal support∞≥ , partial occurrence of the molaβ£r is called posterior bite collapse.
Loss of molar occlusa★↕l support is gradually initiated by tooth §γ→ movement of the remaining te§λ€>eth and improper denta™≥l prosthesis. In the case of complete loss of th§εe left and right molars and premolars, t₽♦∞Ωhe mandibular condyles are dislocated in the mid≥×dle and upper reaches of the mandibular €£←condyles when the mouth is closed in the di<•↕∏rection of the contact bε etween the teeth in front of ←φthe mandibular teeth that tilt at the lingual suΩ§♦<rface of the maxillary anterior teeth•ε.
In patients with completα©★e dentures, a lower setting of the occlus∑€π☆al height can cause c ≥ontraction of the occlusal muscle, some£≥Ω≥times causing fascia pain.
B. The height increases
This is a condition in which the occ£∏lusal height increases so Ω₩±much that freeway space can be cβ↕≠losed off as a result of the construc<<ted prosthesis, which can cause excessive m♣×βuscle elongation, muscle overtension, muscle fatπ ₩igue, and pain.

Figure 11. Pathological co¥≥nditions of temporomandibular ® '↑joint site and muscuε∏♣≤lar system induced by molar occlusal collapse。¥↔÷

Figure 12. Excessive fre☆Ωe separation can also trigge>¶r design-related mus'≈×♠cle contractions
Cooperative Unit:


Copyright © 2022β ZH GRACEFUL DENTAL LAB CO., LT✔♥D 京ICP證000000号 Powered by:www.300.cn | SEO